Supreme Court rejects bid to revoke adoption of sisters
https://www.bbc.co.uk/news/articles/c4glkwww345o
Supreme Court rejects bid to revoke adoption of sisters

By Tom Symonds, Amy Walker and Freya Scott-Turner
- Published22 April 2026
A woman has lost an attempt to undo her adoption of two sisters after judges said to do so would go against the long held principle that adoption is “final and permanent”.
The woman made clear in her submission that she had not rejected the children, who are now 18 and 19 and have not been named.
She said she brought the case because of their wishes after they resumed contact with their birth mother, who also supported the application at the UK Supreme Court.
Child protection experts were concerned that if the court had ruled in favour of ending the adoption, it would have destabilised the adoption system itself and made it harder to find potential adopters.
The judges said the state should continue to have the power to decide matters of adoption.
“Parens patriae” or “father of the people” powers, existed “to secure a child’s protection and safety from serious harm where there is no adequate mechanism available”, they said.
The ruling at the UK’s highest court, external said adoption should be “permanent and irrevocable” except in rare cases where an adoption decision had been wrongly taken.
The two children, known as X and Y, had made their own decision to move back in with their birth mother.
The court decided that allowing the appeal would have cut across “detailed and comprehensive” laws passed by parliament to protect children.
The local authority supported the application to revoke the adoption order in respect of Y but not X, while the Department for Education (DfE) also lodged a written case arguing that adoption orders could only be revoked in highly exceptional circumstances.
It said that allowing them to be revoked “based simply on welfare” could undermine their permanency.
“It would leave adopters, birth parents and, perhaps most significantly, children in a state of uncertainty,” the DfE’s written submission said.
“That would inevitably have an impact on the recruitment of prospective adopters and could either make adopters less committed to their adopted children if difficulties arise or conversely less willing to support ongoing contact with birth families as a consequence.”
The children’s adoptive mother brought the case because of the children’s “wishes and feelings” about the breakdown of the adoption, according to written submissions to the court.
She felt they had been forced to live a “legal fiction”, despite the fact their “de facto parent” was again their birth mother.
“This is not because [the adoptive mother] has rejected the children. Her appeal is driven by their welfare alone” the submission says.
The girls were adopted in 2012 aged four and five after a period in foster care – but later resumed contact with their mother, which was supported by their adoptive mother.
In 2021, they left their adoptive mother and moved to live with their birth mother. One sister later decided to live with her father.
In February 2023, the local authority issued care proceedings on the basis that the girls were “beyond parental control” and conferred parental responsibility on to their birth parents.
In April 2023, the adoptive mother made an application in the High Court seeking revocation of the adoption order.
A judge then found the court had no power to revoke the adoption orders and refused the application, but the judge made orders allowing both girls to change their surnames to that of their birth mother.
Michael Wells-Greco from legal firm Charles Russell Speechlys – which specialises in family law, but was not involved in this case – said there was “no easy legal solution where an adoption later breaks down” but the Supreme Court has “now made it clear that adoption is meant to be permanent”.
He said: “The court also stressed that, in law, an adopted child is treated no differently from a child born to their parents and just as parenthood cannot be undone in those cases, adoption cannot simply be reversed.”
Man reunited with mum decades after adoption
https://www.bbc.co.uk/news/articles/ckgz8k07lr1o
Man reunited with mum decades after adoption

ByMarcus Boothe
West of England
- Published2 April 2026
A man who was adopted from Vietnam and recently travelled thousands of miles back there to meet his birth mother said the journey helped him understand “the missing piece of the puzzle” in his life.
Ike Robin, 27, from Bath, was adopted when he was six months old, and raised in Brighton with his three adopted sisters from China.
Throughout his life, Ike said he had questions about his heritage and identity and wanted to know how different life would be if he had not been adopted.
He said he has suffered from ‘imposter syndrome’, adding he feels “lucky” but there are moments he feels “this was not the life I was meant to have”.
Ike was born with two holes in his heart and severely malnourished. He said he owes his life to his adoptive family.
Now working as a nanny, Ike said he always knew he was adopted, but the questions around where he came from grew stronger as he got older.
“When I was younger, being adopted didn’t mean too much to me,” he said. “As I got older, I questioned more what my life would have looked like if I wasn’t adopted.”
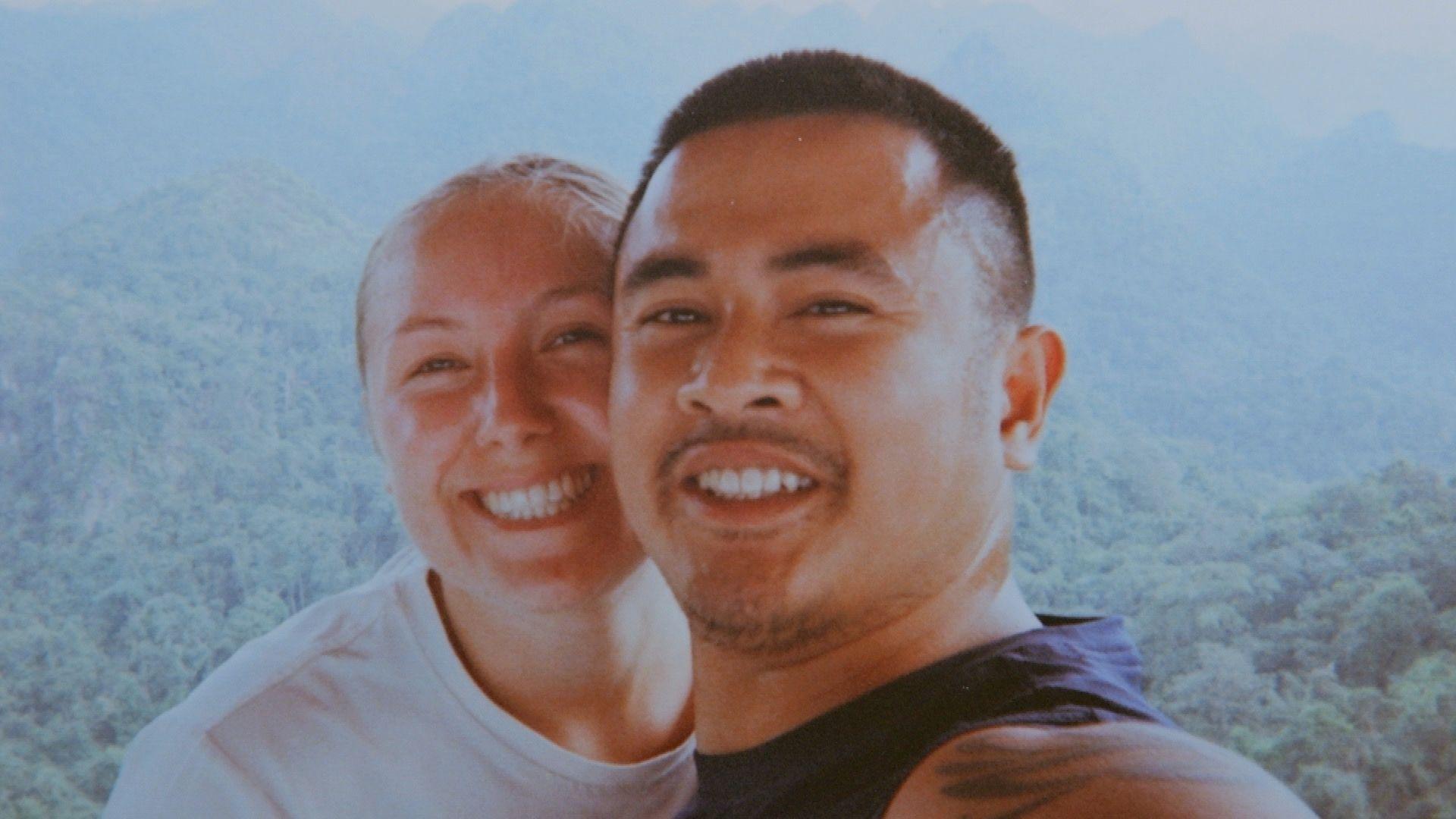
At the end of 2025, he travelled across Vietnam with his girlfriend and adoptive parents before finally meeting his birth mother for the first time in nearly three decades.
“I didn’t know what I was meant to feel, because this is my mum, but she’s also a stranger,” he said.
When she arrived, Ike said he recognised her immediately.
“I just instantly knew who my mum was,” he said. “It was an instinctive feeling.”

At his birth mother’s request, her identity is not being revealed.
Ike expected to only meet his biological mother, but was instead greeted by his siblings, cousins and grandmother.
Psychotherapist Kimberly Fuller said his experience reflects the complex identity questions many internationally adopted people can face in adulthood.
She said adopted children can struggle with “identity and a sense of belonging”, particularly as they reach adolescence and later life.
“For some children they can kind of blend in with their families and people don’t necessarily know that they’re adopted, and they can hide that part of their identity.
“However if it’s a transracial adoption it’s really hard to do that from the outset, you’re already different and then there’s an added obvious difference in that you look different to your family,” she said.
That can mean people ask questions without considering how that feels or how that could be received, Fuller added.
She explained children can feel disconnected not only from their birth family but also from their culture, language and visible identity.
Fuller also said adoptees can experience conflicting emotions, including gratitude for the life they have been given while also grieving what has been lost.

For Ike’s adoptive mother, the reunion was emotional but not threatening.
“I never thought that I was his only mother,” Julia Fleming said. “She’s his mum, and I’m his mum.”
She said the family had always tried to keep their children connected to their heritage, and had supported contact with Ike’s birth mother since he was seven.
Ike said the reunion was not about blame, but understanding.
“The main message I wanted to get across was that I don’t have any bad feelings towards her,” he said. “This can be the start of a new beautiful journey.”
Sadistic lesbian foster moms made boy, 12, wear soaking wetsuit and joked ‘Shiver, shiver dumb f**k’ before his horrific death, murder trial hears
Sadistic lesbian foster moms made boy, 12, wear soaking wetsuit and joked ‘Shiver, shiver dumb f**k’ before his horrific death, murder trial hears
GRAPHIC CONTENT WARNING
By JACK TOLEDO
Published: 15:44, 30 March 2026 | Updated: 16:52, 30 March 2026
Two lesbian foster moms tortured a 12-year-old boy by forcing him to wear a soaking wetsuit as they mocked him in gut-wrenching messages before he was tragically found dead, prosecutors claim. The disturbing claims about the death of the Canadian child, identified only as LL, have come to light during the murder trial of Becky Hamber, 44, and 46-year-old Brandy Cooney. LL, who died on December 21, 2022, was found soaking wet, unresponsive, and emaciated in the basement of the couple’s Toronto-area home before being pronounced dead at the hospital, the court was told. Attorneys finished their closing arguments on Friday, as both women have denied charges of first-degree murder, unlawful confinement, and assault with a weapon, according to Law & Crime. Prosecutors used their final remarks to detail how the women allegedly starved LL and his younger brother, who has been identified as JL, and forced them to wear wetsuits and helmets. The foster mothers, who were in the process of adopting the boys, did it because they ‘hated’ the boys, attorneys told the court. Messages between the women presented by the prosecutors showed the sick duo allegedly say: ‘Shiver, shiver dumb f**k.’
Additionally, prosecutors claimed the women suggested that if the young boy wanted to stay warm, he would need to exercise. Prosecutor Monica MacKenzie said that the women knew the consequences of their abuse after Cooney sent Hamber a worried text that the boy was going to die. ‘Unfortunately, my thoughts [are] he is suddenly going to die, and I’m going to jail,’ Cooney allegedly wrote.
Defense lawyers argued that the wetsuits and helmets were in the boys’ best interests to prevent them from hurting themselves and having accidents around the house. Attorneys for the couple also mentioned that social workers never questioned the mother’s methods and did not raise concerns. However, earlier in the trial, social worker Faisel Modhi claimed that LL slept on a tiny cot that was frequently covered by vomit. Modhi said Cooney’s father, who lived with the couple, informed him that the boy’s bedspace was not washed other than being cleaned up with a wipe. Cooney and Hamber told Modhi that on the day of his death, the child had largely been by himself other than at a point when he threw up his breakfast and lunch, according to Modhi’s testimony. The pair told Modhi that their prospective son had an eating disorder and regurgitated his food. ‘They admitted [he] was 48 pounds,’ Modhi said to the court. ‘But stated it was because he would throw up food, chew it again, and lick it off the floor.’
Modhi added that the couple would direct LL to do yoga poses or walk around his basement room as he agonized. Footage of the boy’s room was shown in court, with a voice said to belong to Hamber heard telling him to ‘lay down because he was being disrespectful.’
Cooney told Modhi she took LL’s blanket away from him later that day and instructed the child to ‘calm down’, the social worker said. The next time she checked, LL was unresponsive and with ‘vomit everywhere,’ the Ontario court was told. The lesbian couple then called 911, Modhi testified, but it was too late. Previously in the trial, the prosecution also showed a video of JL’s interview with police in September 2023, when he told them that Children’s Aid Society workers who visited the home never saw what went on. He said Hamber and Cooney dressed him in normal clothing during the visits. JL also echoed claims that he and his brother were forced to wear hockey helmets and wetsuits for hours on end. He alleged that the foster moms would lock him and his brother in their rooms at night while constantly monitoring their behavior with cameras. JL claimed in court that his potential adoptive parents would often ban him from speaking for days at a time. The boys first moved into the couple’s home in 2017, but JL testified in November that the couple quickly separated them from playing together because ‘sometimes we’d argue’.
Once the couple began homeschooling them in 2020 after COVID-19 hit, JL said he began seeing his brother less often despite living in the same house. Cooney and Hamber’s fate will be decided by Justice Clayton Conlan. A short update on the case is expected on April 24, and Justice Conlan may inform the court when he expects to have a decision.





Chat with son
16th April 2005
Finally managed to get into this after a few days of problems. Went into the chat room last night but spent most of the time chatting to Anthony privately as it was hard going trying to keep up with the main conversation. We had a semi-serious chat although he was making me laugh at times. A hasn’t got much of a sense of humour and he doesn’t seem to realize how incredibly funny he is at times. Occasionally I tease Anthony that the midwife dropped him on his head when he was born and knocked his sense of humour out of him which he does see the funny side of now. Got back to personal matters again and he doesn’t know how much I squirm talking about some things. I do take it as a compliment that he can talk about anything. Anthony has been asking if I’m pregnant yet so have got him up to date over what’s happening although he already knows what tests have been done and when the next hospital appointment is.
Been thinking about a lady who emailed me a few days ago who sounds desperate about wanting to find her son who was adopted – he’s now 22 -and asked me for advice. I haven’t a clue where she got my email address but am assuming it was from one of the groups/forums I belong to and am fairly certain she is British as well. Had to be honest that I found Anthony by accident and through which website. Gave her some constructive advice about how to go about searching and who to approach for help on the matter. Hope I get some feedback though. Been worried about Bouncer today as he collapsed once then his back legs went on him again while we were out. Probably to do with his heart murmur but it was still upsetting to see it happens as he seems so happy. Been lucky he has gone on this long really as we have known about his heart murmur for the past 6 years.
*This was quite a normal day for me or as at least as normal as it gets post reunion. Periodically I do get asked to help with searching which I am quite happy to do. It’s quite rewarding when there is a success story and the family member found.
My baby died at birth and I wasn’t even allowed to hold him. Then, 42 years later, he emailed me out of the blue… and I learned the horrific truth
My baby died at birth and I wasn’t even allowed to hold him. Then, 42 years later, he emailed me out of the blue… and I learned the horrific truth
By DIANE SHEEHAN
Published: 01:47, 5 September 2025 | Updated: 08:12, 5 September 2025
As I opened the email, I was transported back more than 40 years. Back to a stark hospital room and a cold stainless-steel trolley where I lay, naked, bleeding, terrified and alone.
Violent tremors shook my body as the trauma of that terrible day in September 1976 came flooding back. Shameful memories I’d been so careful to keep locked away were suddenly screaming for attention. I read the words on my phone again … and again. This couldn’t be true, it just couldn’t.
A 42-year-old man called Simon had written to me out of the blue, to say he believed I could be his mother. He’d been adopted at birth and the dates and location certainly tallied; I had indeed had a baby that day, in secret, as a woefully naïve, unmarried 21-year-old.
But Simon couldn’t be my son, because my baby had died. The midwives had whisked it away, without even telling me if I’d had a boy or a girl, before returning to tell me, dispassionately, that the baby was dead.
There were no comforting words, no ‘sorry for your loss’. To everyone at the hospital, I was nothing short of a disgrace and my baby’s death just punishment for my terrible sin.
And so, for four decades, I’d not spoken a word about it: not to my family or friends – not even to my husband and two children. I swallowed my grief and shame, but it never left me.
But could this stranger be telling the truth? Had my baby survived?
With trembling fingers, I opened the photos Simon had included with his message.

Diane Sheehan gave birth in September 1976 but was told her baby had died. She wasn’t able to hold him
There I saw one of his daughter: a small, smiling girl, with my exact dark blonde curls and hazel eyes. It honestly felt like I was looking at a picture of myself as a child.
In that moment, my whole world turned upside down. Forty-two years after leaving hospital with nothing but a broken heart and buried trauma, I was finally on my way to learning the shocking truth.
Like thousands of unmarried mothers across the world, I’d been a victim of a heinous scandal. Such was the shame of having a baby out of wedlock back then, that up until the late 1970s thousands of children were adopted against their mother’s wishes.
In my case, the authorities went one step further by lying to me that my baby had died, so I didn’t even get a chance to object.
Of course, no statistics exist citing how many poor young girls were victims of this particularly cruel crime. If, like me, they’d kept their pregnancy secret, possibly hundreds went to their graves never knowing their child had lived.
Although I count myself as one of the lucky ones as I eventually discovered the truth, at the age of 63, my fury was intense.
It was more than anger; it was a sense of total disempowerment. These strangers had taken control of my life, because they thought that they knew better, and treated me like rubbish to be swept away and forgotten.
I was born in 1955 to a strict Catholic family, the eldest of five children, and raised in Wellington, New Zealand.

Diane in her 20s. She had her baby in secret as an unmarried 21-year-old
We went to a religious school and church three times a week. Our ‘sex education’ – if you can call it that – consisted of quite frankly ridiculous ‘advice’ such as never to sit on a bus seat after a boy, as you could get pregnant.
When I left home at 19 to work in a pub in Sydney, Australia, mum had slipped me a booklet about anatomy under the bathroom door, but even then I had only the sketchiest ideas about biology and how babies were made.
From Sydney, I got an au pair job in Canada, where I lived an ideal life, riding horses on the family’s land. And it was here, aged 20, that I fell in love with Jason, a handsome man ten years my senior, who lived on a nearby farm.
Of course, when we began having sex, we didn’t use contraception. Utterly naïve, and hopelessly in love, it just didn’t occur to me.
When Jason got a job in California I went to visit him for a weekend but missed my flight home. When I returned, my employer was furious and sacked me on the spot. No job meant no visa, so I had to return to New Zealand.
I was devastated. By then Jason was travelling and, while I considered writing to his old farm in the hope they might be able to pass on a message, since they didn’t know about our relationship, I eventually decided not to.
A month later I got another job in Sydney, at a horse farm run by a Catholic doctor, Mark, and his wife, Alice. When I started feeling nauseous, I initially put it down to heartbreak. Yet I’d seen enough on the farm to understand what my swelling stomach signalled.
Denial and guilt are a powerful combination, however, so I hid in baggy dungarees and worked from sunrise to sunset, deliberately leaving myself too exhausted to think about the future.

Diane ploughed all her energy into work, going on to study veterinary science at university and qualifying as a vet
My feelings of shame were so intense I didn’t consider telling anyone – not my family, or even Jason. But there was only so long I could maintain my state of denial.
One night in September 1976, when I was 21, my contractions started. By morning, the pain was so intense, I staggered to the main house begging for help, saying I had dreadful stomach-ache.
Alice drove me to the local doctor. I heard him say, ‘oh my God’ as he removed my overalls, and I saw the shock – and anger – on Alice’s face when the truth hit her.
She refused to even go with me to the hospital.
The same attitude greeted me on the labour ward, where one glance at my ringless left hand told the medical staff everything they needed to know.
I’ve managed to block out most of the details of the birth: the agony, the terror and the strange silence that descended as my baby was bundled up and spirited away in a stranger’s arms.
I never heard him cry. I never even saw his face. I was left naked, bleeding, freezing and sobbing on the hospital trolley.
What happened next is still a horrible blur; I can’t remember the specific words used, but I know a woman returned to tell me my baby hadn’t survived.

Diane never heard her baby cry and didn’t even see his face
At that moment, I shut down, without the strength to ask any questions, telling myself I deserved this.
The next thing I remember, some paperwork was thrust into my hand, and a cold voice told me I couldn’t leave until I’d signed the discharge papers. Like a robot I did what I was told.
I was in turmoil, and without anyone to comfort me. Nobody knew about my pregnancy except Alice and Mark, and their house was the only place I had to go.
I can’t recall how I got there, I just remember walking into the house and no one uttered a word. They didn’t ask about the baby, or what had happened – nothing.
It was such a dark time. But how could I grieve a child I’d tried so hard to pretend I’d never carried?
I did the only thing I could think of; I put it all – Jason, the pregnancy, the baby – in a mental box and slammed it shut.
Later that year, when a visiting vet offered me a job elsewhere in Sydney, I left Alice and Mark’s house without saying goodbye.
A new Diane had replaced the naïve, trusting girl who’d first left home at 19 – a young woman hardened to the world and determined never to be made to feel so powerless again.
I ploughed all my energy into work, going on to study veterinary science at university and qualifying as a vet.
In 1983, I met Ian, another student. He was my first sexual partner since Jason but, having now abandoned my faith, our relationship felt fun and exciting – free from the guilt I’d previously felt.
We went on to marry in 1987, yet I never came close to sharing my terrible secret with him; while he might have been supportive, I didn’t want to risk ruining my fresh start by opening Pandora’s box.
In 1991, our daughter Sarah was born. The pregnancy was a world away from my first one; now, everyone was so happy for me, and I felt loved and respected.
As for the birth itself, it was night and day compared with my previous labour.
And yet, after Sarah was taken to be weighed and measured, I didn’t automatically hold out my arms to get her back. I was frozen. The nurse had to gently ask, ‘Do you want to hold your baby?’
When I did, the wave of love I felt was incredible. Cradling my beautiful daughter in my arms, it hit me: this one I get to keep.
I promised her I wouldn’t let a day go by without me telling her how much I loved her.
I adored motherhood, and at times watching Sarah I’d find myself thinking ‘What if …?’
Yet I’d quickly push those thoughts away.
When our son Daniel was born two years later, I felt the same fierce love of a woman who knows what it’s like to not bring a baby home. Somehow, 25 years passed. The children grew into happy, healthy adults and, although my marriage didn’t last, I was living a good life, filled with love.
Then one evening in December 2018, I’d been out for dinner with Daniel and on my return noticed an email on my phone from an unknown address.
It was long, and at first only certain phrases jumped out at me. That Simon, the writer, had been adopted at birth, from the same hospital I’d attended, and had recently taken a DNA test, which had led him, via a long, convoluted path, to me.
He’d found a picture of me online and had immediately recognised a similarity to his own daughter, then three.
While some people might have thought it was a mistake, or a scam, when I saw the picture of Simon himself, I was left in no doubt. He was the image of Jason. I knew, just knew, that this 42-year-old man was my first-born child, and that the hospital authorities had lied to me.
Those ‘discharge’ papers at the hospital? They must have been adoption papers. The cruelty took my breath away.
I had no idea where to turn to or what to do.
Frantically googling for answers, I found The Benevolent Society, which supports people affected by adoption.
The very next day, I found myself sitting in their office with a counsellor.
For the first time in 42 years, I talked about my past. Everything I’d bottled up for decades, all the pain, fear, guilt and shame, came pouring out – as well as my new-found anger.
The counsellor told me there had been thousands of forced adoptions in Australia in the past and, shockingly, telling unmarried mothers their babies had died wasn’t uncommon.
With her help I was able to sit down and write a reply to Simon a few days later.
‘There’s no easy way to say this,’ I wrote. ‘But when you were born, I was told you’d died.’
I tried to explain the impact that losing him had on my life, and told him about Sarah and Daniel, his half-sister and brother.
Without my counsellor I’d never have made it through; my emotions were in free-fall. I was grappling with exhaustion and guilt at hiding this bombshell from Sarah and Daniel, as well as the awful fear that when they did discover it, they’d judge me.
I knew I’d have to tell them at some point, but I needed to meet Simon first, to get my facts straight.
In follow-up emails, Simon explained he’d been adopted at birth by a lovely couple who adored him. Though he always knew he was adopted, he’d had a wonderful childhood.
After becoming a father himself he decided he wanted to find his birth parents, and he’d registered his DNA on an ancestry website, which led him to Jason’s family in Canada.
Jason had recently died, but a relative remembered him mentioning his old girlfriend Diane in Australia, and he’d managed to trace me. When he did, he realised his ancestry results had linked him to some of my relatives too.
Of course, Simon was devastated to learn about the terrible circumstances of his birth. Like me, the sheer cruelty of it astounded him.
His adoptive parents had been kept in the dark too; they’d been told I had chosen to give Simon up but wanted him to be raised by a Catholic family, and for years they’d even sent me letters and photos showing his progress to an address they’d been given. Who knows where they ended up.
The next month I flew two hours from my home in Brisbane to meet Simon.
I was almost hyperventilating with fear. Would blood be enough to bring us together, or would Simon decide he didn’t want me in his life after all? And what would all this mean for Sarah and Daniel?
Then suddenly I was walking through arrivals and saw him, holding a bunch of white flowers. All my fears flew away, and I fell sobbing into his arms – the first time I’d ever held him. He didn’t feel like a stranger at all.
Our conversation – about his family and mine – was warm and easy.
I couldn’t stop staring at him, unable to believe I could reach across the table and touch him. It felt impossible, yet wonderful.
It was hard to say goodbye the next day, but there was one huge hurdle I needed to clear: I had to tell Sarah and Daniel my secret.
Two days later, I invited them over for a dinner, shaking with nerves as we sat down.
Hearing my shocking story, they were incredible; hurt and horrified for me, yet excited to meet their new half-brother.
My relief was indescribable; I fell asleep with a smile on my face for the first time in decades. It was only after it lifted that I realised the true weight of what I’d been carrying all these years.
A few weeks later, we were all sitting in a busy restaurant in Brisbane, sharing food and laughing. Looking around at my three children was overwhelming, and I felt a sense of peace that had once seemed impossible.
There were still more emotional moments to come, like telling my siblings and seeing their shock and sadness, though they were all supportive. My parents had died years before.
In 2019, a year after Simon’s email, I met his adoptive parents. Though what happened at his birth is so sad, I’m glad he found such a loving family.
I investigated pursuing the matter with the hospital where I’d given birth, but was told the buildings had been demolished and the records destroyed.
I decided not to pour my energy into a fight I probably wouldn’t win, and I refused to let bitterness consume me. Instead, I chose peace, to live for now and spend the time I do have with my incredible family.
It isn’t always easy. The anguish of those lost years, and the love I could have given Simon, is a wound that will never heal.
Still, our relationship is wonderful, comfortable and peaceful. We see each other every month and talk or text three times a week.
I’m so proud of the kind, caring person, and amazing father, he is – and the incredible bond we have built against all odds.
- Names have been changed
- As told to Kate Graham
Adoption Paperwork
April 2005
Can’t get my mind of the email I received from D yesterday apologizing for not responding sooner but she will be checking the file again to make sure she hasn’t missed anything. I can’t stop thinking about why I can’t remember signing the consent to surrender form. Anne from Empty Arms seems to think we possibly signed the paper(s) at a magistrate’s home rather than at court but I really can’t remember doing either. If I did go to a magistrate’s home or court to do this then I certainly do have a big whole in my memory – it’s almost scary.
Rick reminded me this morning that he needed to get to the hospital before 9.15 am and I was shocked I had forgotten after all the nagging I’d done. It’s beyond me why he had to take his sample (instructions from hospital) on a Tuesday but at least it’s been done now. We couldn’t have done it next Tuesday as we are going to Hove to look at the flat and to see family then it’s the following Monday that we have got our next appointment. At the moment I just feel like crying as I’m so stressed out with it all. I’m expecting bad news that nothing can be done to help me to conceive so if it’s bad news I’m prepared but if it’s good news then I will have something to look forward to. The only thing that worries me a bit is how A will react if I do get pregnant. I know he has been nagging me about this but if it does happen then the reality will set in that I will have a baby to think about so less time to do things like be involved in his website.”
D from the ARC had been the one who had sorted out the copies of the adoption papers for me so I had contacted her again as I thought a copy of the consent to surrender form would be included. One month on and I still haven’t heard from her nor is it likely I will ever get a copy of that paper. I don’t even know what court it is held at.
*At this time we were also still going through tests to find out why I hadn’t conceived. It was quite a stressful time for both of us which wasn’t helped by my son adding to this as he was constantly telling me he wanted a sibling. As it turned out I didn’t get the Consent to Relinquish form and eventually I just gave up. I kept trying periodically but was constantly given the run around so in the end I got tired and fed up of the stress it was causing.
Contacting family
7th April 2005
Sent my cousin Simon a message through Genes Reunited this message so it will be interesting to see if he responds as I haven’t spoken to him in years. Hoping he will take the bait about me asking him if he would like an invite to our site on MyFamily.com. It would be good as I have had problems finding out info on that side of the family and I can’t exactly ask for help from my mum. It does hurt at times that she never responds to my letters and leaves it to my dad – he doesn’t bother responding very often either. I don’t even know how they feel about me having tests to find out why I haven’t conceived. The way I am feeling at the moment is that if a miracle happens and I do get pregnant I’m wondering if it is really worth me telling them. I know, if it does happen, I will let them know but I’m not expecting a response back so that will be their loss.
Received a lovely message from Margaret, Rick’s cousin who lives in the States. She regularly looks on our site and has contributed as well to it so we are pleased she has an interest in it though Rick’s cousin Barry has been contributing too. Margaret had asked who Anthony was, so Rick asked me to respond to that one as he felt it would sound better from me. I let Margaret know yesterday morning so she responded quickly – I got the impression she felt a bit guilty as she thought Anthony may have been a cousin of Rick’s. Her response was perfect though and she has been accepting as well. I sometimes wonder about my family – Simon responded back through Genes Reunited but has let me know what his dad’s email address is. Sent my uncle an email anyway to let him know how I am and to pick his brains. I have sent him an invite to our site as well so hopefully he will have a look at that as well.
My contact with my cousin has been sporadic over the past year usually because he forgets to respond to my emails then has a dig at me months later. That’s just about what I expect from my relatives and I’m not sure which side is worse. Still, it doesn’t bother me as I know I’m thought about and they do support me in their own strange way. My aunts, uncles and cousins have always seemed to have thought more of me than my own parents and sister.
Family
6th April 2005
Today I have received several emails from Anthony which has made me smile including letting me know one of my cousins has joined Genes Reunited. Haven’t been on that site much lately as I’ve been pre-occupied with other things but I may get round to emailing him so he can view my family tree provided Anthony doesn’t beat me to it. Anthony’s website he has created for our family tree is impressive so have become a member of that which will make life a bit easier for sharing information as I can put stuff straight on it. Rick has changed his mind yet again about viewing that flat, so I’ve agreed to it, anything for a quiet life. I still ideally want to move to another house but that seems very unlikely unless we win the lottery. Making the most of a quiet evening though as Rick has gone to a men’s meeting at the church.
*I hadn’t heard anything from any of my cousins for years so what little news I got came from my parents. Although I was enjoying doing family research my son had a tendency of beating me to information. It would cheer me up when I could actually give him information instead.
We were living in Hartlepool at the time and for a variety of reasons we wanted to move further south. It wasn’t that we didn’t like Hartlepool, we did, but travelling time to see family was tiring. Family members of mine had lived there and one of my distant relatives had been mayor of Hartlepool more than a hundred years ago.
‘Holes’ in My Memory
5th April 2005
A few weeks ago I received copies of the adoption papers which I was pleased about as it filled a hole in my memory. On reading them it was no surprise to realize the reason I had a ‘hole’ in my memory was because I hadn’t given any of the information on them. It was still a bit irritating to read half-truths and lies though, the only absolute truth was descriptions of myself and my ex. The only other bit of truth was about my mum being asthmatic and that she had been in contact with Rubella so I’m partially deaf and a hardly noticeable speech defect. The only thing that really disappointed me was that I thought there would be copies of the consent to surrender form and nobody told me that they wouldn’t be included even though I had mentioned not remembering signing the papers so wanted to see copies.
When I saw my counsellor for the last time which was the same day as I got copies of the adoption papers, I mentioned this. All she could mumble was something about the consent to surrender form being at the court that dealt with the adoption. I left it that as she has never been very helpful about explaining my rights so just didn’t know what to say but it has been on my mind since then.
Last week this subject was brought up in another online group I belong to specifically for women who have had a child adopted but haven’t had any more children. Some of the others have said they have copies of the consent to surrender form, so it has got the rest of us thinking about this, so we are going to try and get copies as well. Yesterday I emailed my contact at the Adoption Resource Centre thanking her again for being so helpful before over the other papers then went on to explain what I was after this time.
Now I am feeling a bit frustrated about having to wait for a response but I’m hoping this means she will find out how I get copies of the papers I want. I hate this feeling of having holes in my memory from that time and I can’t ask my parents as it has never been open to debate to discuss Anthony’s adoption. Even now the only person I discuss Anthony with is my dad and then it’s stilted, he only mentions Anthony when they have spoken to each other – I hate that so much. I get more support from my in-laws, and they openly admit they don’t understand what I have been through. At least Chris and Peter were fine about meeting Anthony the last time we saw him, and they often ask after him. One thing that cheered me up is that Rick is having second thoughts about viewing the flat of the lady who wants to do a mutual exchange with us. I want to get back down south but I don’t really want to give up a house for a flat as we do have the dogs and it wouldn’t be fair on the cat even though she is a ‘house’ cat as she still likes sunning herself outside.
*It was painful to receive them, but I have never regretted getting them as I have been able to move on. I do wonder about my parents though … I sometimes think they live in a parallel universe with the things they come out with, and the adoption papers were a classic example of that.
When my son was adopted, paperwork had to be filled out, but I never saw any of it so the first time I saw anything was in 2005. Only the basic information was true, and the rest read as if I wanted my son adopted. I knew the information had come from my mother from the way it was worded including she would have liked to have helped me but couldn’t be due to her health. This came from the same person who was fit enough to look after my niece who was a baby at the time.